"It is important to recognize that Gilead’s licenses are a wolf dressed as a lamb. They will hinder access for millions of people in desperate need of HCV treatment, and harm the entire generic industry"
Tracy Swan, Hepatitis/HIV Project Director at Treatment Action Group in New York City.
Globally, an estimated 185 million people have HCV [4]. Each year, nearly 500,000 of them die from HCV-related complications, such as liver cancer and liver failure [5]. But hepatitis C can be cured, which dramatically reduces the risk of liver-related illness and death. In clinical trials of sofosbuvir and ledipasvir, the combination has demonstrated high cure rates and improved safety and tolerability, compared to the previous standard of care.
Gilead claims their priority is to “increase access to its medicines for people who can benefit from them, regardless of where they live or their economic means,” [6] but their HCV license actually creates a barrier to universal access by excluding many middle-income countries (MICs) and high-income countries (HICs), by controlling generic competition and segmenting markets. Even in countries where generic sofosbuvir can be sold, if Gilead fails to register its drug and get regulatory approval in that market, the drug cannot be made available there. Therefore, the license does not guarantee access even in the countries included in the geographical scope of the license.
Myth: Gilead is making sure that everyone who needs affordably-priced, generic sofosbuvir will have access to it.
Fact: This license leaves out nearly 73 million people with HCV who will have to pay Gilead’s high prices.
HICs and MICs such as China, Brazil, Russia, USA, Thailand, Turkey, Mexico, Ukraine and Georgia have some of the world’s highest HCV prevalence rates. These and other HICs and MICs represent nearly 73 million people with HCV – Gilead has not included them in their licensing agreements, because Gilead sees them as profit-making “commercial” markets. See the list of countries excluded from Gilead’s VL
Nearly three quarters of the world’s poor, who largely pay for healthcare out of pocket, live in MICs. Millions of people who need HCV treatment will not have access to generic versions of Gilead’s HCV medicines, the generic versions will be more affordable than the price their governments will get through direct negotiations with Gilead.
While HICs and MICs account for 88% of the global HCV epidemic, Gilead’s license covers primarily low-income countries (LICs) in Sub-Saharan Africa, South and Southeast Asia and island nations, many of which have little to no HCV prevalence data or treatment demand.
Myth: Gilead is making agreements with generic companies that will increase access to sofosbuvir in LICs and MICs.
Fact: Gilead is locking down deals with generic producers to control – and limit – where sofosbuvir can be sold
Gilead is including countries in the VL as a strategy to:
Prevent competition with non-licensee generic producers: In reality, Gilead’s license will prevent sales of the active pharmaceutical ingredients (API) used as raw materials for local production to non-partners of Gilead, even in countries included in the license. "This is terrible news for countries who have capacity to produce their own medicines," said Othoman Mellouk, Regional Advocacy Coordinator of ITPC in The Middle East and North Africa (MENA), "In countries like Egypt where 20 million people are infected with HCV, governments will not be able to secure treatment for all even with the discounted price provided by Gilead. The country started working recently on local production of sofosbuvir to ensure sustainability of treatment. Now, with this license, local manufacturers will not be able to buy APIs anymore from Indian suppliers. Egypt will now have to completely rely on generic producers selected by Gilead - which essentially means just replacing a monopoly with another. Although this country is covered by the license and the patent on sofosbuvir is not granted, free and fair generic competition is just not possible anymore, thanks to Gilead’s move." Read ITPC press release
Block the sale of sofosbuvir outside the license territories, despite pending sofosbuvir patent oppositions. Patient advocates and generic companies have filed multiple sofosbuvir patent oppositions in India, but Gilead’s license undermines their impact. Even if the Indian courts reject the key patent, licensees in India will not in reality sell or export sofosbuvir to non-licensed territories.
Control the market even where there is no patent protection: The Gilead license allows seven Indian drug companies to market generic versions of sofosbuvir and ledipasvir in the 91 territories covered by the license. Yet, in many of the included countries — particularly LICs— Gilead’s drugs are not patent-protected. This means that a country could technically buy the drugs from any available source.
For countries excluded from the license
The seven Indian generic companies that have signed Gilead’s 91-country license are most of the generic producers that are able to compete with Gilead (Read the letter to Cipla endorsed by 49 civil society organizations). Yet, they have agreed to a highly restrictive license that prevents them from selling sofosbuvir and ledipasvir, even in countries where:
No patent has been filed or granted
A patent is pending
Patent oppositions and patent invalidations have been successful
For example, the governments of Brazil (2.6 million with HCV), Thailand (1.5 million with HCV) and Morocco (625,000 with HCV) cannot buy the generic sofosbuvir that will be produced in India by the seven companies licensed by Gilead — although there is no patent on sofosbuvir yet granted in these countries. These and other countries with large HCV epidemics are victims of a Gilead monopoly, and DAAs will be unaffordable for the majority of people with HCV in these countries.
Myth: Gilead says that their reduced US$900 price per course of sofosbuvir is fair.
Fact: The same amount of sofosbuvir can be produced—profitably—for US$ 101.
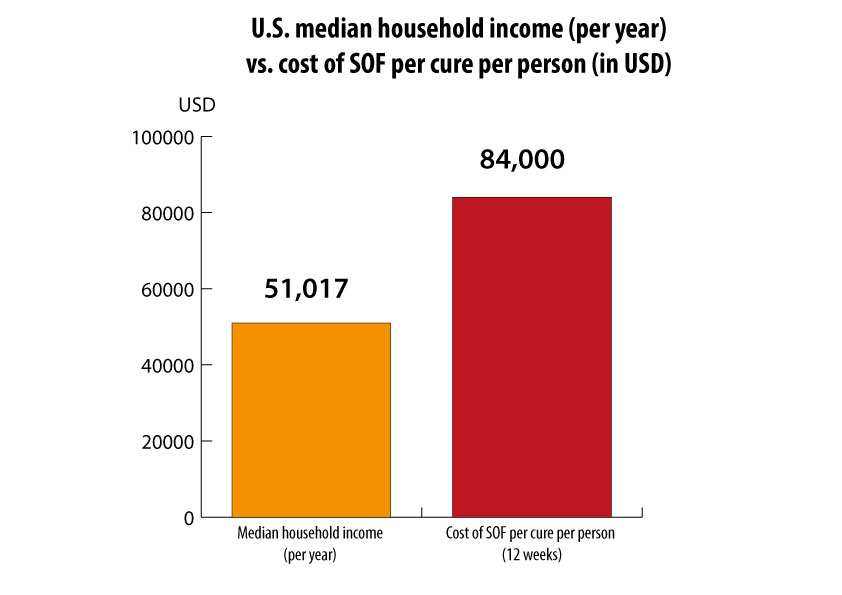
Gilead has priced sofosbuvir at US$84,000 for a 12- week treatment course (US$1000 per pill). It must be used with other drugs — and some people may require a 24-week course— making HCV treatment even more expensive. Gilead charges, US$900 for 12 weeks of sofosbuvir in certain low-income countries. But sofosbuvir can be profitably mass-produced for about US$101. Ledipasvir, one of the DAAs used with sofosbuvir to treat genotype 1, could be mass-produced for only $93.
Sofosbuvir can also be used with other non-Gilead HCV DAAs, such as daclatasvir (from Bristol-Myers Squibb) —which can be mass-produced for US$20. [7]
Sofosbuvir pricing in high-income countries
The astonishingly high price of sofosbuvir—US$84,000 for 12 weeks of treatment in the US; currently 56,000 euros in France (US$ 71,300) – is a barrier to access. Sofosbuvir’s price has generated debates about sustainability. In HICs, this price has led to treatment rationing and exclusion of key populations: in many places, treatment access is limited to those with late-stage disease, or denied to people who use drugs or alcohol. Though inadequate access to sterile injection equipment has led to millions of HCV infections among people who inject drugs, HCV treatment is being unfairly withheld from this high-prevalence population. Research demonstrates that people who inject drugs have similar treatment adherence, completion and cure rates to non-users [8] [9]. Withholding treatment from certain groups based on prejudice should never be tolerated for any disease.
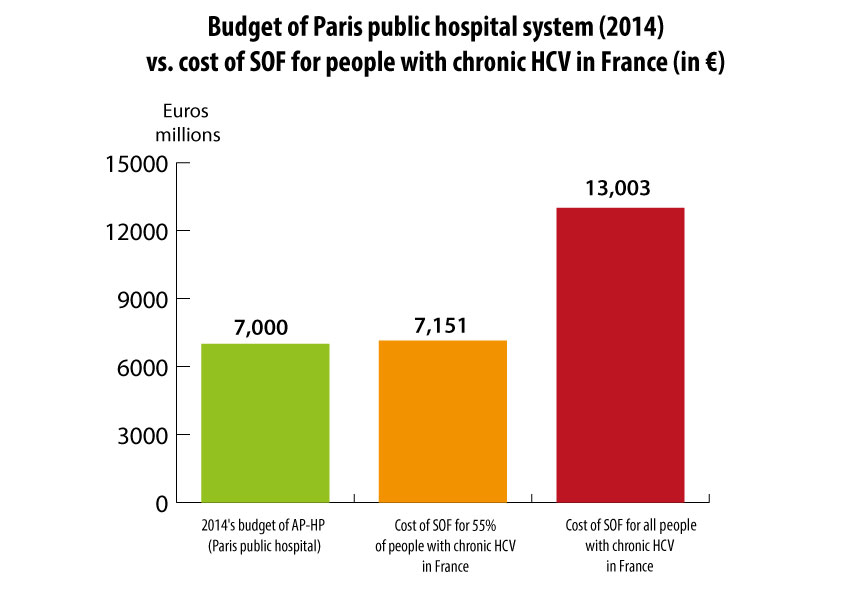
In early 2014, the first expert report on hepatitis C in France was published and recommended treatment with DAAs for people with a chronic hepatitis C with fibrosis stage ≥ F2 (127,700 persons in France). Treating all of these people with a sofosbuvir-based regimen would cost more than the entire 2014 budget for the Paris public hospital system—just for sofosbuvir. And recently the independent public authority– la haute autorité de santé (HAS) – changed these recommendations and endorsed prioritization of people with more serious liver disease stage ≥ F3. A collective of French civil society organizations, to avoid this rationing, asked the government to issue a compulsory license in order to get affordable generic sofosbuvir. Read the press release
In the US, an expert guidelines panel has recommended prioritizing treatment for people with advanced liver disease and severe extrahepatic manifestations. Unfortunately, public and private payers have used this as a rationale for refusing to treat people, without medical evidence to justify their criteria.
What will the price of sofosbuvir be in middle-income countries that were excluded from the license?
Sofosbuvir’s price will likely be significantly higher than the US $900 price given to Egypt, particularly in the private sector (where insurers or employers may pay for treatment).
I-MAK has analyzed the cost implications of the licenses announced by Gilead Sciences on the Hepatitis C drug sofosbuvir. The 3 page report is available here.
In Thailand, 1.5 million people have HCV (2.2% of the total population). Yet, Thailand was excluded from Gilead’s license. The Thai government’s universal healthcare scheme covers the cost of HCV treatment, but Gilead’s decision to exclude Thailand means the government must pay at least US$ 121 billion —instead of US$ 1.3 billion (the estimated generic version price under the license)—for sofosbuvir. This price is about 15 times higher than Thailand’s entire annual health budget (USD $8.4 billion) in 2014. Read Thai civil society’s press release
In Brazil, due to Gilead’s pending patent application, the government opted to negotiate prices exclusively with Gilead. While there is no official information, local experts expect that price for 12 weeks of sofosbuvir will be about US$ 7,000 in Brazil. This is 52 times more expensive than the generic version could be, and adds at least US$ 1 billion to the cost of treating all people with HCV in Brazil. Read Brazilian civil society’s press release
In Morocco, access to treatment for its 625,000 people infected with HCV appears seriously compromised, because the country is excluded from Gilead’s license. In Morocco, the cost of treatment is not borne by the health system, nor can most people with HCV pay for these treatments out of pocket. Morocco’s exclusion from Gilead’s license will cost the Moroccan government at least US $790 million to treat its people. Read ITPC-Mena Press release
Prices for middle-income countries included in the license
Inclusion in Gilead’s license does not equal universal access; in included territories, sofosbuvir will still be priced well above the actual cost of manufacturing the drug profitably. Also, Gilead will receive a particularly high royalty of 7% on all sales of the generic versions.
Gilead has said it would charge US $300 for one month’s supply of sofosbuvir in India. Yet, HCV genotypes 1 and 3 ( the most common in India), require six months of treatment, bringing the cost to US$1,800—not including the other drugs that must be used with sofosbuvir.
Egypt is the only MIC with whom Gilead has finalized a price for sofosbuvir. The Egyptian government purchases it for US $900 (per 12-week course) for use in the public sector, though Gilead may cap the number of treatments it sells to Egypt (where an estimated 11 million people have HCV). Treating HCV genotype 4, the predominant strain in Egypt, requires 24 weeks of sofosbuvir (US $1,800) plus another medication. All the Egyptians who won’t be included in the national program must pay for their HCV treatment out of pocket for drugs on the private market. The price of sofosbuvir will be nearly 6 times more expensive (US $9,000 – $10,800) than the government price; since Egypt’s gross national income per capita per month is slightly more than US $260 [10], the private sector price is prohibitive for most Egyptians.
Conclusion
As the HIV epidemic demonstrated, unrestricted generic competition improves access to essential medicines more effectively than industry-driven approaches, such as voluntary licensing or tiered pricing (where a company charges higher prices in some countries). From early 2000 until 2010, generic competition led to a 90 percent price reduction of key HIV/AIDS medications over a decade.
Gilead’s license is a fool’s bargain that inhibits access for nearly half the world’s HCV population. While they restrict access to life-saving medications, Gilead will be reaping an undue profit in poor countries that desperately need these essential medications.
It is unclear when people with HCV in countries included in the Gilead license will actually receive treatment; in many places, it will take at least 2 years for generic sofosbuvir to become available.
Gilead’s license is undermining rights countries have under international law (also called TRIPs flexibilities) to utilize public health safeguards such as compulsory licensing or defining its own patentability criteria.
Sofosbuvir’s registration - approval by each national regulatory authority for each medicine is an inescapable process. But in most countries—including the Eastern European/Central Asian (EECA) region where HCV is rampant - Gilead has not publicized their plan or timeline for registering sofosbuvir (Read EECA CAB open letter to Gilead). This remains a barrier to access for most of the countries.
Next steps
Silent Protest organized by the Delhi Network of Positive People (DNP+) and the Indian Drug User Forum (IDUF) during Gilead’s press conference on September 14
Governments have to take all available measures under global trade rules and national patent laws to secure access to low-cost generic versions of HCV medicines.
Governments and treatment advocates must identify Indian generic companies willing to produce sofosbuvir and sell it to countries outside the Gilead license territories.
Treatment advocates should continue to hold Gilead and other DAA producers accountable for preventing access to life-saving HCV medicines.